In most societies, doctors enjoy very high levels of privilege, status, and respect. This entails expectations that they be competent, altruistic, and moral. For this status to be maintained, a harmonious relationship between the medical profession and the society it serves is necessary.
But in many parts of the world, including India, this relationship is under significant stress; recent studies and systematic reviews highlight the rise in violent attacks on doctors and healthcare workers globally.
Types of violence experienced by doctors in India
As part of our study, we conducted a detailed content analysis of Sakal, a leading local language (Marathi) newspaper, to examine how violence against doctors is represented in the media. This analysis, and our in-depth interactions with doctors and healthcare managers, suggests that violence against doctors manifests in multiple, interrelated forms. These range from subtle coercion, where doctors feel compelled to make decisions that compromise their professional judgment, to overt acts of hostility. The latter includes verbal abuse and humiliation by aggrieved patients or their families, as well as physical assaults such as shoving or hitting.
Also significant, though often under-acknowledged, is defamation: the public slandering or malicious accusations that can inflict reputational harm. In the absence of reliable and comprehensive statistics to systematically map contemporary trends (in India and globally), it remains difficult to accurately quantify the extent of the problem; however, our analysis suggests that the situation is getting worse in India and globally.
The underlying dynamics need further attention
Crucially, our analysis indicates that the violence we see is merely the tip of the iceberg, and that, regardless of measurement-based assessments of the extent and gravity of the situation, underlying dynamics demand in-depth scholarly attention and critical examination. This paper seeks to explore how such an inquiry might be most fruitfully undertaken in the present context.
This topic has been receiving significant scholarly attention. Figure 1 presents the trend for papers (approx. 500) with the terms ‘doctors’ AND ‘violence’ in the title, indexed in Pubmed.
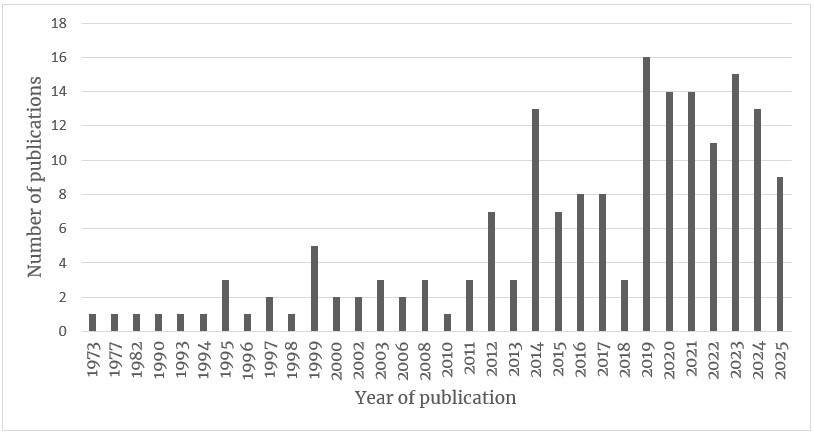
Figure 1: Numbers of papers by year. Source: Authors.
A scan of the abstracts suggests that an in-depth examination of this social phenomenon is necessary. According to a survey conducted by the Indian Medical Association in 2015, more than 75 percent of doctors had experienced some form of violence in the course of their work, with 12 percent reporting incidents of physical assault. These figures are particularly alarming when juxtaposed with global estimates from the World Health Organisation, which suggest that between eight percent and 38 percent of healthcare workers worldwide encounter physical violence at some point in their careers.
Drivers of violence against doctors
Over the past three years, we have conducted a field-based inquiry using India as a case study. Employing a range of methods, including media content analysis and in-depth qualitative fieldwork, we have developed a nuanced understanding of the issue. Our analysis suggests that the rise in incidents of violence against doctors is not an isolated phenomenon or merely a matter of law and order, but rather a manifestation of deeper structural and relational transformations within the health system and society in India, with parallels, albeit in different stages of evolution, in many other parts of the world.
These changes include, but are not limited to, the growth of misinformation across all social spheres, the commercialisation, corporatisation, and managerialisation of the health system, and the related financial strain that day-to-day healthcare use entails in the Indian context. At its core is also the growing disjuncture between societal expectations of how healthcare ought to be provided and the day-to-day and current realities of care provision. Our analysis leads us to argue that to better understand this phenomenon, one must examine it in light of the state of the medical profession and the state of the social contract between the medical profession and the society it serves. Crucially, we found that this phenomenon demands an analytical lens that moves beyond a reductive victim–perpetrator binary.
The social contract between the medical profession and society
We contend that the complexities of this phenomenon can be meaningfully unpacked through examining the following key elements of the relational arrangement between society and the medical profession: expectations, trust, social identity, and social conflict. This draws on empirical findings from our research in India, scholarly writings about professions generally (and the medical profession specifically), and research from across the world on the relationship between society and the medical profession.
While we have prioritised these four, research from other parts of the world also points to a range of other factors, such as commercialisation of healthcare, regulatory ecosystems, media representations, technological transformations in medical practice, and broader political-economic shifts, which may also shape this relational arrangement between the medical profession and society. However, our research in the Indian context has led us to foreground these four interrelated dimensions as analytically central and encompassing of other factors. Importantly, each of these elements do not operate in isolation; rather, they are deeply interwoven. Shifts in one domain (e.g., expectations) frequently reconfigure others (e.g., trust or conflict). At the same time, their cumulative interactions may generate or intensify identity crises among medical professionals, which, in turn, reshape the domain of expectations and recalibrate trust. Together, these processes produce a dynamic, mutually constitutive relational field.
Expectations within the doctor-patient relationship
There is a vast body of research on the doctor-patient relationship, which suggests that patients now have different and increasingly higher expectations from the medical profession, in part driven by a discourse of technological developments in medicine, and the marketisation and commodification of healthcare. Globally, the traditional social expectations that doctors should offer competent, ethical care are being extended to include the expectation that doctors deliver successful recovery and that doctors should provide good customer service. While current research highlights the centrality and importance of expectations, the researcher and medical doctor Mehmet Cetin et al. are the only researchers (to our knowledge) to have explicitly examined the expectations that patients now have of their healthcare providers.
Cetin and his colleagues do not, however, examine the expectations the medical profession might ‘now’ have of society—society understood broadly to include social structures and institutions, including but not limited to the health system of which healthcare providers are an integral part. Our field inquiry around the phenomenon of violence allowed systematic exploration of expectations as they stand now, reasons for changes to the ‘expectations’ of the parties involved, i.e., society (broadly and its various constituents) and the medical profession.
We found a mismatch of expectations between society and medical professionals, shaped both by the contemporary market-driven organisation of healthcare in India and by the historically entrenched notions of professional roles and responsibilities. This mismatch, we contend, provides critical insights into the rise in incidents of violence against doctors and also into the shifts occurring in the social contract between the medical profession and society.
Trust of doctors by patients
Trust serves as another key element of the relationship between society and any profession, but particularly the medical profession. Trust is a multilayered concept including both cognitive and affective elements, although primarily it involves the trustee having positive expectations about the trustor’s intentions and competence, i.e., the trustor shares the interests of the trustee, and the trustee is confident in the trustor’s competence to produce the expected outcomes. Trust forms an essential basis for the harmonious functioning of this relationship; it has been argued that unless citizens can trust the health system that serves them, population level health outcomes cannot be improved. As Bloom et al observe, ‘trust is central to the social contract of the medical encounter and affects numerous dimensions of the relationship’.
Many scholars have noted the erosion as well as the reconfigurations occurring in trust in the relationship between the medical profession and society. This research highlights how this reconfiguration is shaped within the context of the changing state of the medical profession, transformations in health systems, and, more broadly, the economy and society. We contend that unpacking various aspects of trust relations between doctors and patients (interpersonal trust), society, and the medical profession (institutional trust) can help shed light on the violent unraveling of the social contract.
The professional identities of doctors
A key feature of the functioning of a social relationship is the identities of those involved. Studies about the social and professional identities of doctors (both the formation and maintenance of these identities) offer many useful entry points to study the state of the medical profession in a society at a point in time. There are studies that highlight how individual doctors draw on collective ways of thinking within and about the medical profession to form and maintain their identities. There is also research that examines identity formation and maintenance in different societies and cultures and advocates for context-specific approaches to understanding professional identity formation and maintenance. Then there is research that mobilises different theories of identity development and maintenance to examine the relationship between society and various professions. For example, medical educator Dr. Helmich and colleagues draw on psychological approaches and relational sociological approaches to unpack how personal, role, and group identities amongst medical practitioners shape their interactions and relations with members of society.
Consistent across these different ways of looking at social and professional identities is the notion that identities are not static and that they change and evolve. As identities evolve, so do their relationships. Consistent across researchis also the notion that actors often wear multiple hats and that different identities are invoked and mobilised at different times. These different identities are often at odds with each other, which compels doctors to ‘juggle’ multiple identities, resulting in the broader reconfiguration of the medical profession’s identity. We contend that examining the identities of medical professionals along the above lines and within the broader context of the changing identities of the people they serve can offer valuable insights into the phenomenon of the rise in violence against doctors, and the state of the medical profession in society.
Social conflict
Another aspect that stands out in research pertains to the state of a society broadly i.e., the state of important societal institutions and how they relate to each other and to members of society. We would expect that these broader relational arrangements and dynamics also impinge upon the relationship between the medical profession and society. We contend that the conflictual aspects of the relationship between doctors and patients, and more broadly the medical profession and society, can be usefully understood using understandings of social conflict articulated by sociologists Lewis Coser and Louis Kriesberg. Coser argues that any social system involves an allocation of power and status positions among sub-groups of actors in the system and that all relations reflect the outcome of ongoing contestation and negotiation between different groups in society for privilege and status. Coser adds, ‘There is never complete concordance between what individuals and groups within a system consider their just due and the system of allocation.’ As groups contest and grapple for allocation of power (power to and power over) and status, conflict ensues when an impasse or a state of unresolvable disagreement occurs.
Drawing on Coser’s point that conflict provides a ‘means for avoiding the ossification and ritualism’ within social institutions (like medicine) and that social conflict ‘though apparently dysfunctional for highly rationalised systems, may actually have important latent functional consequences,’ we contend that a careful examination of the nature and drivers of the social conflict between the medical profession and society can offer valuable insights towards resolving the impasse and towards reconfiguring this critical relationship.
In our field inquiry in India, we examined the conflict between society and medical professionals through the lens of social anger. Our findings suggest that perceived breaches of the social contract, widespread misunderstandings about the organisation and functioning of the health system, and the absence of effective grievance redressal mechanisms create the conditions for a low threshold for the violent expressions of anger.
As Figure 2 below shows, the key elements outlined above, i.e., expectations, trust, social identity, and social conflict, coalesce around and can be usefully studied within the broader frame of the ‘social contract’ between the society and its medical profession.

Figure 2: A framework for studying the relationship between the medical profession and society. Source: Authors.
The Social Contract
Every society fashions its own agreements, explicit or tacit, about the rights and duties of different members—these agreements are necessary for the smooth conduct of social life and relations within societies. This ‘contract’ involves an agreement amongst members of a society to uphold and abide by some basic social rules, laws, institutions, and/or principles of conduct. A reading of the works of key social contract theorists, i.e., Hobbes, Locke, and Rousseau, suggests that this agreement amongst citizens and institutions within a society is arrived at through tacit and explicit deliberations towards establishing the bases for diverse groups with different expectations and diverse social status to cooperate, negotiate, and agree. The bases can vary widely. They are often associated with notions of fairness, morality, propriety, reciprocity, and rationality, but can equally concern power, privilege, and domination. Since these deliberations are about agreeing to basic social rules, laws, institutions, and/or principles of conduct, they require some form of trust, but they can also sometimes be disagreeable, even violently so.
A well-functioning social contract and a harmonious relationship between the medical profession and the people it serves is essential for a country’s health system to fulfil its mandate. Scholars across the world have been observing changes and reconfigurations in this social contract and have been trying to make sense of these changes. Medical sociologist John McKinlay has famously talked of the ‘end of the golden age of doctoring’, while others have highlighted the struggles around the redistribution of power and financial control between professionals and managers within how healthcare is provided. Others still see the shifts in patient-doctor relations as a functional democratisation of relations amidst broader social reconfigurations, growing social distances, and reducing information asymmetries. Recent analysis emphasises the importance of the changes in the governance and regulation of the medical profession, the rise of managerialism, and the corporatisation of healthcare. Medical sociologist Michael Calnan argues that what we are seeing is, in fact ‘a reconfiguration of professional power’ generally.
Social contracts are dynamic and are in a perpetual state of negotiation and flux. Within this understanding, we argue that the stress in the social contract between society and the medical profession can be understood as a feature of the interaction (and disconnects) between ideas about the nature of the social contract and the changing realities of society and the healthcare system. To specify, traditionally and historically, interactions between doctors and patients have involved a paternalistic dynamic, where doctors require patients to suspend their usual claims to the integrity of their intimate experiences and of their bodies, and doctors decide for patients and tell them (i.e., prescribe) what patients should do. This authority primarily accrues from the doctor’s unique access to specialist knowledge and expertise. Today, easier access to this specialist knowledge through higher levels of literacy in society and greater access to the internet contributes to a reconfiguration of this authority, particularly the paternalistic aspects of this authority. This authority also accrues from the doctor’s historical, traditional, and deeply entrenched status as the all-knowing and benevolent healer.
Today, the doctor-patient relationship is more than ever seen as that between a client and a service provider and is increasingly framed within market logic as any other service transaction. In many parts of the world, this framing has been formalised in law, and we contend that this is also potentially contributing to a demand for reconfiguration of doctors’ authority, particularly the paternalistic healer aspects of their authority, and also has implications for the violent unraveling of the social contract with the medical profession in many societies. In the Indian context, this strain in the relationship between medicine and society has largely been interpreted through a law-and-order framework or has been reduced to a victim–perpetrator binary. In contrast, we offer a more constructive, non-polarising approach to examining this important societal relationship. We contend that such an approach enables a more nuanced examination of the specific socio-institutional conditions shaping this relationship, not only in India but also in other contexts where similar dynamics are emerging.
Conclusion
Drawing on insights from the Indian context, we argue that to comprehensively understand the rise in violence against doctors, and to effectively address the health systems concerns it triggers, one needs to examine the phenomenon in light of the broader state of the medical profession and the state of the social contract between the medical profession and society, across different country contexts.
Authors: Prof. Sumit Kane and Dr. Mayuri Samant.
Main image: Photo by Imad Clicks.



